


Translator: Rhonda Jacobs
Reviewer: Leonardo Silva This is me ten years ago. I weighed 40 pounds more than today, and like many people,
I wanted to lose weight. Like many people, I wanted to know
what is the best diet for humans. Many of us actually have an opinion
about this question. Some believe that a low fat,
plant-based diet is the best. Others, that a low-carb diet, rich in protein
and animal fat, is the best. Others have opinions
on how much sugar we should eat, or how much salt, cholesterol,
saturated fat, eggs or dairy products we should have in our diet. But the question of what the best diet is, is a scientific one, so there should be no room
for opinions or beliefs. If Diet A is really better than Diet B, then a study that compares
the two on enough people should show that definitively. No opinions, no beliefs,
just hard data, right? What is also clear is that
if the best diet does exist, then we haven't yet found it because the incidence
of diet-related disease has increased dramatically
in the past several decades. Now, you might think it's because
people don't listen to what we tell them.
But in fact, that's not true, people actually generally
do follow dietary guidelines. But according to
the Center for Disease Control, if you live in the United States, there's over a 70 percent chance
that you're either overweight, diabetic or have non-alcoholic fatty-liver disease. And there's overwhelming evidence
that diet and lifestyle are major drivers of these conditions. So why is it that after so much research, we still don't have an answer
to the seemingly simple question of what is the best diet for humans? What I'd like to propose to you today
is that the reason we don't have an answer is because we've been
asking the wrong question.
And it's the wrong question
because it assumes that the best diet depends
only on the food and not on the person eating it. But what if differences in our genetics,
lifestyle, our gut bacteria cause us to respond differently to food? What if these differences explain why
some diets work for some people but not for others? What if our nutrition needs to be
personally tailored to our unique make-up? This is exactly the question
we set out to ask in our own research, which I did with my colleague Eran Elinav and several graduate students
from the Weizmann Institute of Science. To take a scientific approach, we first searched for a metric
of healthy nutrition that we should study. Most studies examine weight loss
or risk of heart disease after some diet. But the problem is that these are affected
by many factors unrelated to diet, they take many weeks to change, and in the end, you get
a single measure of success. And if it didn't work, well then
it's very hard to understand why.
And so instead, we searched for a metric that would still be relevant
for weight management and diet-related disease, but one that we could also easily
and accurately measure across many people. And this led us to focus
on blood glucose levels, and more precisely, changes
in blood glucose levels after a meal. We call this a "meal glucose response." Why is it important? Well, because high
glucose levels after a meal promote both hunger and weight gain. After we eat, our body digests the carbohydrates
in the food into simple sugars and releases them into the bloodstream. From there, with the help of insulin, cells throughout our body
remove the glucose from the blood so that they can use it
as a source of energy. But insulin also signals our body
to convert excess sugar into fat and store it, and that's a primary way
by which we gain weight. In addition, fast flow
of glucose into the blood often causes our body
to release too much insulin, which could lower our glucose levels
to below baseline, making us feel hungry and eat more.
Meal glucose responses
are also very relevant for our health because they've been shown
to be risk factors for obesity, diabetes, cardiovascular disease
and other metabolic disorders. A recent study that followed
2,000 people for over 30 years found that higher meal
glucose levels after meals predict overall higher mortality. Finally, and not least important,
with recent technological advances, we can now follow a person's
glucose levels continuously for an entire week.
And since the average person
eats around 50 meals a week, it allows us to measure glucose responses
to 50 meals in just a single week. Meal glucose responses also provide us with a way to directly measure
the effect of every single meal, as opposed to common approaches that only evaluate
the effect of an overall diet. Now, of course, there are many factors
beyond glucose levels that influence a healthy diet. But this is a very important one, and solving it
can be a major step forward. Luckily for us, we managed to convince
1,000 healthy people of this idea, and we connected them
to one of these small glucose sensors and tracked their glucose levels
continuously for an entire week. And during that week, participants
logged everything that they ate on a mobile app that we developed. And so that allowed us
to measure glucose responses to 50 different meals for each person and around 50,000 different meals
across all 1,000 participants, making our study the largest one that was ever done
on this problem until today.
So what did we find? Well, when we looked
at averages, we saw trends. For example, more
carbohydrates in the meal generally increase the response. This is not so surprising. Another, perhaps more surprising, trend is that more fat in the meal
generally decreased the response. But – and this is
the key finding of our study – for every trend we found, there were many people
who were very different from it. Basically, when the same person
ate the same meal on different days, the response was very similar.
But when different people
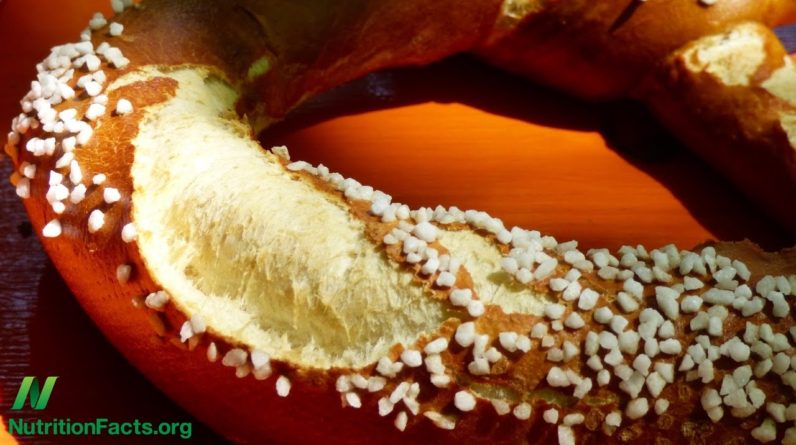
ate the same meal, the response was very different. For example, white bread
induced almost no effect on the blood sugar levels of some people, but in others, it induced huge spikes. And the same was true
for every single food we tested, including rice, pizza,
sushi and even chocolate. For every food, there were some people
who had low responses, others who had medium responses, and yet others
that had very high responses. It wasn't just about the food, it was also about the person eating it. So while averages
and trends are informative, for any given individual,
they may not mean much. Now, it wasn't just about
how good the body was at handling sugar, each person had different foods
that spiked his levels. Some people even had opposite responses. For example, some people
spiked for ice cream but not for rice.
But then others spiked for rice
and not for ice cream. In fact, more people spiked for rice
than for ice cream. Now, my wife is a clinical dietician, so when I showed her
this data, she was shocked, because as a practitioner, she of course
relies on general dietary guidelines, and so one of the first things that she tells her many
newly diagnosed pre-diabetics is to stop eating foods such as ice cream and instead eat more
complex carbohydrates such as brown rice. So, as soon as she saw our data, she of course realized
that for most of her patients not only does her dietary advice not help, but in fact, it pushes them faster
to develop the very same disease that her advice was meant to prevent. So these results of ours
on such a large data set convinced us that responses
to food are personal, and that diets that maintain
normal blood glucose levels must therefore be personally
tailored to the individual.
They also show, in our view,
why the current nutritional paradigm that searches for that one best diet
is inherently flawed. The best diet for humans does not exist. Our responses to food are personal, so our dietary advice
must also be personal. And personalized dietary advice
was our next challenge. To tackle it, we measured
many parameters across participants that we thought may explain
people's variability in glucose response to meals. And these included basic metrics
and lifestyle factors like age, weight, height and physical activity, but also blood tests, medical background
and food frequency questionnaires, and also DNA sequencing
of both the human genome and the gut bacteria composition
of each person. Now, of these, the gut bacteria was perhaps the most novel
component that we examined. For hundred of years, we know
that bacteria live within our body. But only with recent advances
in DNA sequencing could we begin to study them extensively.
And when we did,
we found that this vast collection of hundreds of different species
that we each host, collectively termed "our microbiome," has a major impact
on our health and disease. And what makes the microbiome
even more exciting is that unlike our genetics,
we can also change it even by simple means,
such as changing what we eat. Our bacteria help us digest
some of the food that we eat, and in turn, produce molecules
that are taken by our own cells and affect our physiology. For example, in our own research,
we studied artificial sweeteners, which the vast majority of us
consume on a daily basis in various diet soda drinks
and other products. And we found that consumption
of artificial sweeteners alters the composition of the gut bacteria
such that when transferred into mice causes the mice
to develop symptoms of diabetes. And so this and several other studies led us to ask whether the microbiome
would also be important for explaining people's
glucose variability in response to meals. And so we took this microbiome
and other clinical data that we collected, and we used advanced
machine learning algorithms to automatically search for rules that predict personalized
glucose responses to meals.
For example, one such rule could be that if you're over 50,
and you have a certain bacterial species, then your response
to a banana will be high. The overall algorithm
combined tens of thousands of such rules that it automatically
deduced from the data. This approach is actually similar to how websites like Amazon
make book recommendations, except that we applied it
to how people respond to food. And we could show that this algorithm
could then take any person, even people who are not part
of our original study, and predict the response
to arbitrary meals with high accuracy. So as a final step, we asked
whether we can also use this algorithm to design personalized diets
that normalize blood glucose levels. So we recruited
and profiled new participants, and we asked the algorithm to predict
two diets for each person; in one diet, which we called
the "bad diet," we asked the algorithm to predict foods for which that person
would have high responses. And in the other – "good diet" – we asked it to predict foods for which
that person would have low responses.
And each person then followed
each diet for one week. Now, by design, the diets
had to be identical in calories. In fact, all breakfasts,
lunches and dinners had the same calories on different days. And it's also important to note that each person received
a different personalized diet, and there were even some foods that were given to some people
on their good diet but to others on their bad diet. Now, to show you that these diets are not the obvious ones
you might think of, here they are for one of our participants. Now, take a moment and see
if you can guess for yourself which one the algorithm
predicted to be the good diet and which to be the bad diet
for this particular participant.
And as you look at these,
notice that each diet contains foods that would not typically appear
in standard diets. And now for fun,
let's play a quick guessing game, and you all have to participate. So, raise your hand if you think
the diet on the right is the good one. Okay. Now raise your hand if you think
the diet on the left is the good one. Okay, definitely we see
nearly a 50/50 split here, showing you that
it's definitely not trivial to guess. And I can tell you
that for this participant, the algorithm predicted
the diet on the right, the one with the ice cream,
to be the good one. And so now the only question is
how good did these diets work. And what I'll show you next is in our view perhaps the most striking result
that came out of our study. So here are the continuous glucose levels of this participant
when following the bad diet. And you can clearly see abnormally high
glucose levels after meals indicating that this participant
has impaired glucose tolerance and is likely pre-diabetic.
But on the good diet,
the one with the ice cream and the same amount of calories
as the bad diet, this same pre-diabetic participant
achieved fully normal blood glucose levels without even a single spike
across the entire week. Obviously, we were very happy
to find out these results, and, in fact, we found similar results
for most participants for which we designed personalized diets
using our algorithm. Now, not only that, but the good diet
also induced several consistent changes in the gut bacteria of most participants. And it seemed that
these changes were beneficial, because bacteria that in other studies
were associated with good outcomes tended to increase after the good diet, and bacteria associated with disease
tended to decrease. And this result is of course
very intriguing because it suggests that in addition
to normalizing blood glucose levels during the intervention week, the good diet also induced
beneficial effects that may persist even beyond
the intervention week. So what's the take-home message
from all of this? Well, based on the glucose
responses variability that we saw across 1,000 people, our conclusion is that
there is no single best diet for humans because we are all too different.
It also means that if
a certain diet hasn't worked for you, then maybe it was the wrong diet for you. Your dietary failures
may not be your fault. Your diet may have failed simply because it did not take information
about you as an individual into account. So what can you do
with this information now? Well, right now, you can actually measure your personal glucose responses
to your favorite meals using simple glucose devices
that you can buy at your local drug store. And I guarantee that you'll be surprised at which foods personally spike
your glucose levels and which do not. As a more complete solution, we are working hard to make
our algorithms available to everyone so that you'll be able, from your home, to provide basic
clinical information about yourself, send a sample of your microbiome, and in return receive
personalized dietary advice.
We are also starting longer-term
dietary intervention studies in both pre-diabetics and diabetics
that will go on for a full year. Because we believe that if the effect
of normalizing blood glucose levels that we were able to obtain in one week
could persist for a longer time period, then we might be able to reverse,
and even cure, these conditions, which constitute one
of the worst epidemics of our times. More broadly, I believe that we are entering
a new era in the study of nutrition, one in which we will move away from asking
what is the best diet for humans, and instead, focus
on the more appropriate question of what is the best diet for me.
Thank you very much. (Applause).