

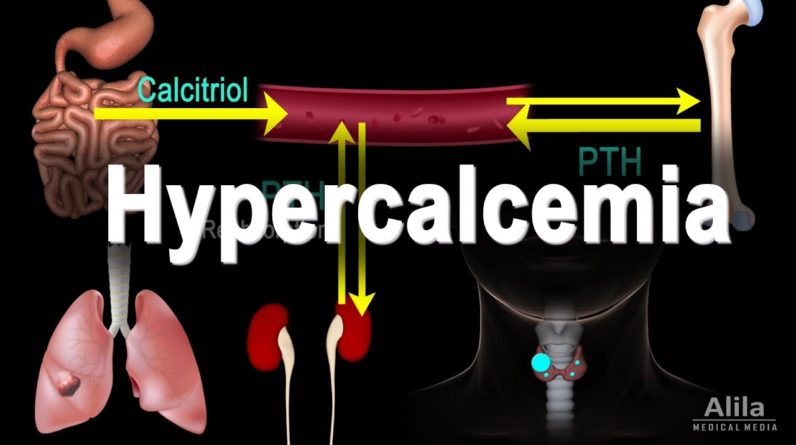
Hypercalcemia refers to abnormally
high levels of calcium in the blood. Dietary calcium enters the blood through the
small intestine and exits in urine via the kidneys. In the body, most calcium is located
in bones, only about 1% is in the blood and extracellular fluid. There is a continual exchange
of calcium between blood serum and bone tissue. The amount of calcium in circulation is mainly
regulated by 2 hormones: parathyroid hormone (PTH) and calcitriol.
PTH is produced in the parathyroid
gland while calcitriol is made in the kidney. When serum calcium level is low, PTH is upregulated.
PTH acts to promote calcium release from bones and reduce calcium loss from urine. At the same
time, it stimulates production of calcitriol, which promotes absorption of calcium in the small
intestine while also increases reabsorption in the kidney. Together, they bring up calcium levels
back to normal. The reverse happens when calcium level is high. This feedback loop keeps serum
calcium concentrations within the normal range. Hypercalcemia is generally defined as serum
calcium level greater than 2.6 mmol/L. Because the total serum calcium includes albumin-bound
and free-ionized calcium, of which only the latter is physiologically active, calcium levels
must be corrected to account for albumin changes. For example, increased albumin levels produce
higher serum calcium values but the amount of free calcium may still be normal. On the other
hand, in conditions with low blood pH, albumin binds less calcium; releasing more free calcium
while the total serum calcium may appear normal. Most symptoms of hypercalcemia can be
attributed to the effect it has on action potential generation in neurons.
High levels of
extracellular calcium inhibit sodium channels, which are essential for depolarization.
Hypercalcemia therefore reduces neuronal excitability, causing confusion, lethargy,
muscle weakness and constipation. In most cases, excess calcium in the blood is a direct result
of calcium release from bones as they break down, becoming weak and painful. As the kidneys
try to get rid of the extra calcium, more water is also removed, resulting in dehydration,
excessive thirst and kidney stones. Extremely high extracellular calcium may also affect cardiac
action potentials, causing arrhythmias.
Typical ECG findings include short QT interval, and
in severe cases, presence of Osborn waves. While hypercalcemia may result from a variety
of diseases and factors, hyperparathyroidism and cancers are responsible for about 90% of
cases, with the former being by far the most common cause. In hyperparathyroidism,
PTH is overproduced due to benign or malignant growths within the parathyroid gland.
An existing cancer elsewhere in the body can cause hypercalcemia in 2 major ways. First, some
cancer cells produce a protein similar to PTH, called PTHrP, which acts like PTH to increase
serum calcium. Unlike PTH, however, PTHrP is not subject to negative feedback; consequently,
calcium levels may keep rising unchecked. Second, cancers may spread to bone tissues,
causing bone resorption or osteolysis, and subsequent calcium release into the blood.
Hypercalcemia treatment consists of lowering blood calcium levels with a variety of drugs, and
addressing the underlying cause. While treatment outcome for hyperparathyroidism is generally
excellent, prognosis for malignancy-related hypercalcemia is poor, possibly because it
usually occurs in later stages of cancer..